|
|
|
|
Lake Forest Hospital
Glucose Management LFH Endocrinology Pager: Anthony Pick 5-9476 Dr. Liz Kunreuther: 5-7725 Dr. Disha Narang: 1-9731 Dr. Harjyot Sandhu 16553: (August 2020) Theresa (Terry) Wojciak APN, CDE: (April 2020) Mary Wehmeyer Inpatient RN CDE Anthony Pick, MD CDE Contact: [email protected] Mobile: 773-495-8909 Spok pager 312-695-9476 | ||||
|
Notify/Consult Endocrinology/Diabetes educator:
ALL Type 1/DKA prone patients New onset diabetes +/- symptoms +/- high A1c At risk of readmission for glucose related issues Insulin pump use DKA/HHS U-500 insulin use Severe insulin resistance (high doses, > 1 u/kg/day) High dose steroids + diabetes/hyperglycemia Diabetes + tube feeds + hyperglycemia Severe or persistent hyperglycemia Unpredictable insulin needs Hypoglycemia < 54 mg/d Hypoglycemia unawareness Admission for symptomatic or severe hyperglycemia (A1c > 10%) Complex diabetes - gastroparesis, renal transplant, advanced complications Diabetes + pregnancy + medical admission Glucose management: Gold standard: Basal insulin + Rapid acting insulin with meals + Correction Scales-see tables In general, stop all oral agents, non insulin injectables Check A1c (if none in 90 days and no transfusions etc.) Monitoring: Point of care glucose before meals, bedtime (default) Consider 2drive.google.com/open?id=1tjbH2OEJfKlIs02Mr_-syi4jdCTv49RVAM check: bedtime correction, high dose steroids, risk of hypoglycemia, unstable glucose patterns LIMIT OR AVOID "SLIDING SCALE" INSULIN AS FAR AS POSSIBLE NEVER USE SLIDING SCALE ALONE IN DM1/DKA PRONE Diet or oral agent controlled (current A1c < 7%) diabetes: Short-term correction scale may be acceptable initially Insulin treated diabetes, DM1, DKA prone, glucose > 180: LONG ACTING + RAPID ACTING: MEALS + CORRECTION Document and assess home regimen: hypoglycemia, hyperglycemia, total daily dose of insulin (units/kg/day) Goal blood glucose: fasting/pre-meal 100-140 mg/dl, random or post-meal < 180 mg/dl is default Prevention of inpatient DKA Notify endocrinology of ALL DM1, DKA prone patients NEVER omit basal insulin in DM1/DKA prone Follow insulin pump protocol If insulin pump stopped ALWAYS provide basal long acting insulin SQ (unless appropriate for IV insulin infusion) Use standardized protocol for glucose > 400 mg/dl Measure rapid turnaround beta-hydroxybutyrate assay per protocol Respond to falls in bicarbonate and/or rise in anion gap Criteria for use of IV insulin DKA/HHS Diabetes OR stress hyperglycemia > 180 mg/dl + Critical illness OR cardiogenic shock High dose steroids + persistent or severe hyperglycemia Unpredictable SQ insulin needs Glucose > 600 mg/dl ICU Glucose target 140-180 mg/dl |
Routine SQ Insulin dosing:
Long acting (glargine) + Rapid Acting insulin (Lipro) with meals + Rapid Acting (lispro) Correction Scales Calculate Total Daily Insulin Dose (TTD) by weight: Patient category per table, multiply factor by weight in Kg Divide TTD into 50% basal and 50% mealtime (divide with 3 meals) If patient on insulin at home (basal, basal-meal, 70/30): Compare calculated dose with 80% of total home dose and always use the LOWER of 2 doses e.g. 75 kg (0.4 u/kg/day): 75 x 0.4 = 30 units TTD 50% glargine = 15 units Meals: 5 units lispro Correction: low dose (<40 units/day) meal default: 60-75g consistent carbohydrate diet Type 1 diabetes/insulin deficient diabetes Consider basal + insulin:carbohydrate ratio with meals + correction scales e.g 1:15 in women, 1:10 in men default Assuming 60g meal = 4 units in women, 6 units in men
Preexisting diabetes: Insulin orders
long-acting +meal rapid acting (as appropriate) + Correction Correction alternative: 1-5 units per 100 mg/dl starting with glucose > 150 mg/dl 1:100 (1) 1:50 (2) 1:35 (3) 1:25 (4) 1:20 (5)
|
Value |
LOW (1:50) |
MEDIUM (1:30) |
HIGH (1:20) |
CONFIGURABLE 1:100, 1:75, 1:15, 1:10,1:5 |
150-199 |
1 |
1 |
2 |
*** |
200-249 |
2 |
3 |
4 |
*** |
250-299 |
3 |
5 |
7 |
*** |
300-349 |
4 |
7 |
10 |
*** |
350-399 |
5 |
9 |
13 |
*** |
> 400 |
See severe protocol |
- |
- |
- |
1:100 |
1:75 |
1:25 |
1:15 |
1:10 |
1:5 |
|
150-199 |
0 |
0 |
2 |
2 |
5 |
10 |
200-249 |
1 |
1 |
4 |
6 |
10 |
20 |
250-299 |
1 |
1 |
6 |
10 |
15 |
30 |
300-349 |
2 |
2 |
8 |
13 |
20 |
40 |
350-399 |
2 |
3 |
10 |
16 |
25 |
50 |
> 400 |
See severe protocol |
- |
- |
- |
- |
- |
JUST INSULIN DAILY
Watch BG trends:
IF BG> 140 mg/dl fasting OR > 180 mg/dl random, increase TTD 10-20%
If BG < 100 mg/dl, decrease 10-20%
Increase mealtime insulin if BG values elevated at pre-lunch, pre-dinner, or bedtime
Increase basal insulin: If fasting BG > 140 mg/dl AND BG drops less than 50mg/dl from bedtime to fasting
Alternative: Take 50% of prior 24 hours correctional insulin, 1/2 basal, 1/2 with meals
Insulin sensitivity factor estimate: 1500/TTD (1500-1800/TTD)
Insulin: carbohydrate ratio estimate: 500/TTD (300-500/TTD)
SPECIAL NUTRITIONAL SITUATIONS
NPO or clear liquids
Do not hold basal insulin (especially DM1)
Consider decreasing basal insulin by 20% (DM1), up to 50% (DM2) (see preoperative protocol)
Use weight based TTD per table, give 40% as basal
Do NOT give mealtime insulin, use appropriate correction scale
Meals
Default is consistent carbohydrate of 60-75g
Carbohydrate counting: Insulin: carbohydrate ratio (number of units per g carbohydrate
Example: 1:10 I:C ratio: 6 units to cover 60g of carbohydrate, male default 1:10, female default 1:15)
Tube feeds:
Nocturnal: Basal 1/d, rapid with start cycle, add correction, BG 4/day
Bolus: Basal 1-2/daily, rapid 3-4/day (hold NPO), BG 4/day: add rapid correction
Continuous: Basal 1-2/day, regular Q6(hold NPO), rapid Q4, BG 4/d, add rapid correction
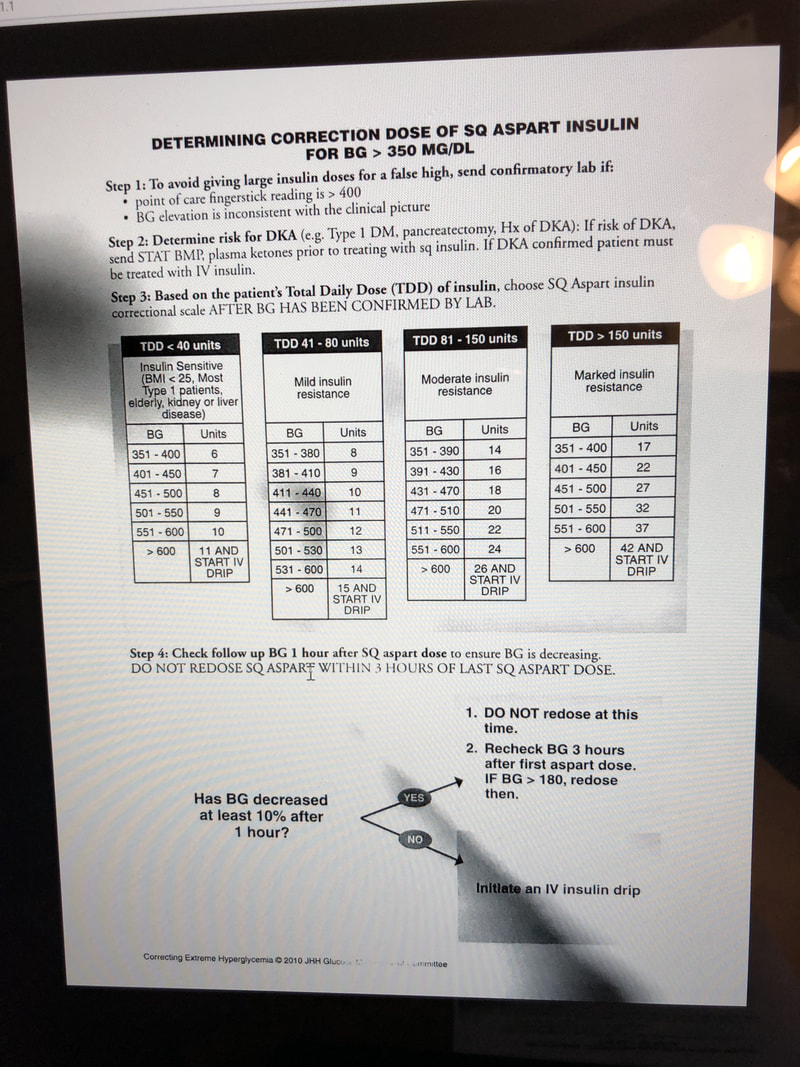
SEVERE HYPERGLYCEMIA > 400 mg/dl
Hold food, encourage non-glucose containing fluids (unless fluid restricted)
Rule out DKA/HHS (stat basic chemistry, beta-hydroxybutyrate): transfer ICU if confirmed, sustained glucose > 600 mg/dl
Assess for spurious result, assess for causative factors (stress, high carbohydrate intake)
Check steroid use: see steroid protocol
Option 1: Give correction of rapid acting insulin 5-10% of weight based TTD per table (peaks in 1-2 hours)
Avoid stacking by separating doses by at least 3 hours
Can check at 1 hour (check at least 10% drop)
Option 2: starting glucose-110/correction factor (at least one step up from current correction scale)
Example: Glargine 24 units, meals, 8 lispro per meal, medium dose correction (1:30-35), Glucose 460 mg/dl
480-110/25 (high dose scale correction) = 350/25 =14 units rapid acting insulin SQ
STEROID-INDUCED HYPERGLYCEMIA
Convert steroid to prednisone equivalent:
prednisone 20mg = methylprednisolone 16mg = Dexamethasone 3mg
Prednisone > 100mg daily, consider endocrinology consult
Insulin naive or prednisone < 40mg
If steroid dosed daily: Add NPH 10 units with steroid dose
If steroid doses multiple times daily, add rapid acting insulin e.g. lispro 3 units with each meal
Adjust dose 10-20% daily as needed
Insulin resistant or prednisone dose > 40 mg
Prednisone equivalent(mg)-20/20 x 0.1 units x body weight (Kg)
Maximum initial single dose: 20 units, insulin naive, 40 units insulin experienced
Give NPH with each steroid dose
If giving evening steroid, order 3AM glucose check
Alternatives:
1.Basal-bolus-correction (weight based TTD: 50-50% basal + meals (1/3 per meal) + correction
2. OR give 30% basal, 70 % meals (20-40-40%) + correction
Total daily dose 0.5-0.6 (or higher: 0.7-1.2+ U/kg/day)
Adjust at least 10-20% daily
Option 3 Prednisone 10mg NPH 0.1 u/kg/day, 20mg=0.2, 30mg=0.3, >40mg 0.4 u/kg/d
Option 4 use 130% of home insulin dose initially, frequent adjustments as needed
Watch BG trends:
IF BG> 140 mg/dl fasting OR > 180 mg/dl random, increase TTD 10-20%
If BG < 100 mg/dl, decrease 10-20%
Increase mealtime insulin if BG values elevated at pre-lunch, pre-dinner, or bedtime
Increase basal insulin: If fasting BG > 140 mg/dl AND BG drops less than 50mg/dl from bedtime to fasting
Alternative: Take 50% of prior 24 hours correctional insulin, 1/2 basal, 1/2 with meals
Insulin sensitivity factor estimate: 1500/TTD (1500-1800/TTD)
Insulin: carbohydrate ratio estimate: 500/TTD (300-500/TTD)
SPECIAL NUTRITIONAL SITUATIONS
NPO or clear liquids
Do not hold basal insulin (especially DM1)
Consider decreasing basal insulin by 20% (DM1), up to 50% (DM2) (see preoperative protocol)
Use weight based TTD per table, give 40% as basal
Do NOT give mealtime insulin, use appropriate correction scale
Meals
Default is consistent carbohydrate of 60-75g
Carbohydrate counting: Insulin: carbohydrate ratio (number of units per g carbohydrate
Example: 1:10 I:C ratio: 6 units to cover 60g of carbohydrate, male default 1:10, female default 1:15)
Tube feeds:
Nocturnal: Basal 1/d, rapid with start cycle, add correction, BG 4/day
Bolus: Basal 1-2/daily, rapid 3-4/day (hold NPO), BG 4/day: add rapid correction
Continuous: Basal 1-2/day, regular Q6(hold NPO), rapid Q4, BG 4/d, add rapid correction
SEVERE HYPERGLYCEMIA > 400 mg/dl
Hold food, encourage non-glucose containing fluids (unless fluid restricted)
Rule out DKA/HHS (stat basic chemistry, beta-hydroxybutyrate): transfer ICU if confirmed, sustained glucose > 600 mg/dl
Assess for spurious result, assess for causative factors (stress, high carbohydrate intake)
Check steroid use: see steroid protocol
Option 1: Give correction of rapid acting insulin 5-10% of weight based TTD per table (peaks in 1-2 hours)
Avoid stacking by separating doses by at least 3 hours
Can check at 1 hour (check at least 10% drop)
Option 2: starting glucose-110/correction factor (at least one step up from current correction scale)
Example: Glargine 24 units, meals, 8 lispro per meal, medium dose correction (1:30-35), Glucose 460 mg/dl
480-110/25 (high dose scale correction) = 350/25 =14 units rapid acting insulin SQ
STEROID-INDUCED HYPERGLYCEMIA
Convert steroid to prednisone equivalent:
prednisone 20mg = methylprednisolone 16mg = Dexamethasone 3mg
Prednisone > 100mg daily, consider endocrinology consult
Insulin naive or prednisone < 40mg
If steroid dosed daily: Add NPH 10 units with steroid dose
If steroid doses multiple times daily, add rapid acting insulin e.g. lispro 3 units with each meal
Adjust dose 10-20% daily as needed
Insulin resistant or prednisone dose > 40 mg
Prednisone equivalent(mg)-20/20 x 0.1 units x body weight (Kg)
Maximum initial single dose: 20 units, insulin naive, 40 units insulin experienced
Give NPH with each steroid dose
If giving evening steroid, order 3AM glucose check
Alternatives:
1.Basal-bolus-correction (weight based TTD: 50-50% basal + meals (1/3 per meal) + correction
2. OR give 30% basal, 70 % meals (20-40-40%) + correction
Total daily dose 0.5-0.6 (or higher: 0.7-1.2+ U/kg/day)
Adjust at least 10-20% daily
Option 3 Prednisone 10mg NPH 0.1 u/kg/day, 20mg=0.2, 30mg=0.3, >40mg 0.4 u/kg/d
Option 4 use 130% of home insulin dose initially, frequent adjustments as needed
Prednisone dose |
NPH: insulin naive or sensitive |
NPH: insulin resistant or experiences |
40mg |
20 |
40 |
30mg |
15 |
30 |
20mg |
10 |
20 |
10mg |
5 |
10 |
5mg |
5 |
5 |
INSULIN PUMP:
Notify endocrinology
Do NOT use if: unstable, no supplies, mental status changes, suicidal, psychosis, not proficient
Use signed contract/waiver when implemented (see updated policy)
Hypoglycemia: Rx < 70 mg/dl, incident report < 40 mg/dl, with adverse clinical effects
15g carb (4 Oz. juice,soda, 8 oz. non-fat milk, 3-4 glucose tablets), recheck Q20 mins until > 70 mg/dl. If unable to take PO: 25 ml of D50 IV = 25g (consider glucagon, D10)
Ultra long acting insulin: Toujeo(U-300 glargine), Tresiba(degludec)-adjusted every 3-4 days. Optimal dose adjustment prior to surgery not clearly defined
Care with SGL2i (Cana-dapa-empa-gliflozins) as associated with (euglycemic) DKA
Perioperative/NPO: Insulin treated diabetes cut basal 80% night before (type 2 diabetes with poor oral intake consider 50%), 50% basal on day of surgery (unless ultra long axcting)
Critical illness: Glucose goals: 140-180, IV insulin protocol, Check glucose hourly (use lab or blood gas glucose for poor perfusion, pressors)
High risk Surgery: Check A1c. Check glucose before, during or just after surgery, before PACU Discharge. Correction insulin for glucose > 150mg/dl. Basal-meal-correction after surgery. See detailed protocol
Discharge planning/transition of Care:
Aim to identify patients who will need insulin on discharge early in admission
Check insurance coverage and access to follow up (PCP versus endocrine)
For patients with access barriers:
Erie Clinic in Waukegan (federally funded formulary and staffed with help of LFH Family Medicine Residents)
Lake County Clinic (larger operation than Erie, federally funded formulary and may have a diabetes nurse)
Work with case management and social work as needed
Suggest use EMMI education videos and nurses to teach glucose monitoring and insulin injection (pens and/or vials)
Insulin discharge planning checklist:
Meter, test strips
Insulin
Syringes and/or pen needles
Glucose tablets
Urine ketone strips
Alert ID
Hand out and understanding on diagnosis and treatment of hypoglycemia:
Rule of 15; 15 g carb, recheck in 15 minutes = 4oz. juice, regular soda, glucose tablets, 8 oz. mild etc.
Follow up plan.
Suggest "meds to beds" with LFH Walgreens as can check what is covered and affordability
Relion brand meters test strips, vials of insulin most affordable usually
70/30, regular and NPH are $25 a vial range from Walmart, Target etc
Can check pricing on GoodRx.com
Lantus (glargine): biosimilar is basaglar (often less expensive)
Humalog: biosimilar as admelog
Check if pens versus vials covered by insurance and check affordability
Check that patient and or family can safely inject insulin, use meter and recognize and treat hypoglycemia
Usual insulin regimen options:
Basal + meals + correction
Basal + largest/dinner meal +/- corrections
Basal alone
NPH to cover prednisone (see steroid protocols)
70/30 twice a day
Notify endocrinology
Do NOT use if: unstable, no supplies, mental status changes, suicidal, psychosis, not proficient
Use signed contract/waiver when implemented (see updated policy)
Hypoglycemia: Rx < 70 mg/dl, incident report < 40 mg/dl, with adverse clinical effects
15g carb (4 Oz. juice,soda, 8 oz. non-fat milk, 3-4 glucose tablets), recheck Q20 mins until > 70 mg/dl. If unable to take PO: 25 ml of D50 IV = 25g (consider glucagon, D10)
Ultra long acting insulin: Toujeo(U-300 glargine), Tresiba(degludec)-adjusted every 3-4 days. Optimal dose adjustment prior to surgery not clearly defined
Care with SGL2i (Cana-dapa-empa-gliflozins) as associated with (euglycemic) DKA
Perioperative/NPO: Insulin treated diabetes cut basal 80% night before (type 2 diabetes with poor oral intake consider 50%), 50% basal on day of surgery (unless ultra long axcting)
Critical illness: Glucose goals: 140-180, IV insulin protocol, Check glucose hourly (use lab or blood gas glucose for poor perfusion, pressors)
High risk Surgery: Check A1c. Check glucose before, during or just after surgery, before PACU Discharge. Correction insulin for glucose > 150mg/dl. Basal-meal-correction after surgery. See detailed protocol
Discharge planning/transition of Care:
Aim to identify patients who will need insulin on discharge early in admission
Check insurance coverage and access to follow up (PCP versus endocrine)
For patients with access barriers:
Erie Clinic in Waukegan (federally funded formulary and staffed with help of LFH Family Medicine Residents)
Lake County Clinic (larger operation than Erie, federally funded formulary and may have a diabetes nurse)
Work with case management and social work as needed
Suggest use EMMI education videos and nurses to teach glucose monitoring and insulin injection (pens and/or vials)
Insulin discharge planning checklist:
Meter, test strips
Insulin
Syringes and/or pen needles
Glucose tablets
Urine ketone strips
Alert ID
Hand out and understanding on diagnosis and treatment of hypoglycemia:
Rule of 15; 15 g carb, recheck in 15 minutes = 4oz. juice, regular soda, glucose tablets, 8 oz. mild etc.
Follow up plan.
Suggest "meds to beds" with LFH Walgreens as can check what is covered and affordability
Relion brand meters test strips, vials of insulin most affordable usually
70/30, regular and NPH are $25 a vial range from Walmart, Target etc
Can check pricing on GoodRx.com
Lantus (glargine): biosimilar is basaglar (often less expensive)
Humalog: biosimilar as admelog
Check if pens versus vials covered by insurance and check affordability
Check that patient and or family can safely inject insulin, use meter and recognize and treat hypoglycemia
Usual insulin regimen options:
Basal + meals + correction
Basal + largest/dinner meal +/- corrections
Basal alone
NPH to cover prednisone (see steroid protocols)
70/30 twice a day
|
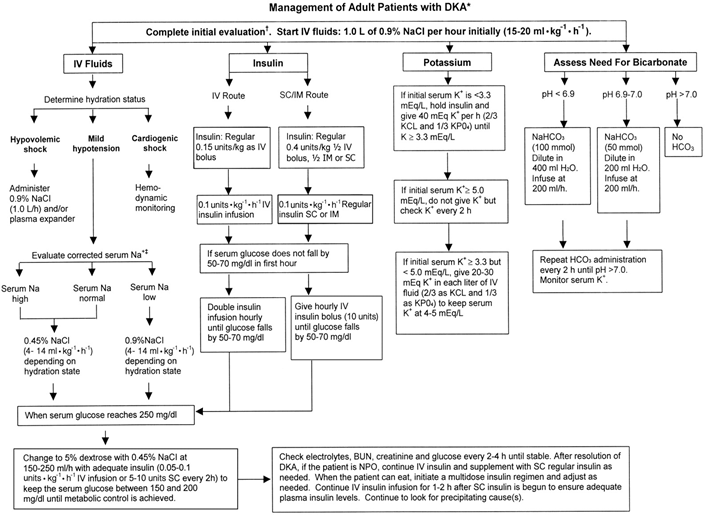
Lake Forest Hospital DKA/HHS Management 2018:
See Policy and order sets Notify: Endocrinology (Page 1-9755), Nephrology for ARF, advanced CKD, ESRD DKA Prevention: NEVER omit basal insulin in type 1 diabetes/DKA prone/insulin pumps Diagnosis of DKA/HHS: Diabetic Ketoacidosis (DKA), Hyperosmolar hyperglycemic state (HHS)can overlap: Look for triggers-infection ischemia, non-adherence, social factors, pump problems DKA glucose usually > 200 mg/dl, pH <7.3, C02 < 15 MeQ/l, Anion Gap > 12, Beta hydroxybutyrate > 3.0 Meq/L, ketones positive (moderate pH < 7.24, severe < 7.0) HHS BG> 540-600, pH > 7.3, Bicarb> 18, BHB <3.0, ketones small-zero, mOSm/kg > 320 Predicted fluid and potassium deficits: Water deficit DKA 7-14 Liters HHS 10-22 Liters!! Potassium deficit DKA 210-350 mmol/kg HHS 350-1050 mmol/kg DKA Initial Studies: HbA1c, Basic chemistry, Magnesium, Calcium, Phosphate, Blood gas (venous or arterial) Beta Hydroxybutyrate (or ketones): rapid turn around approved CBC, Amylase/Lipase Osmolarity, Urinalysis (others-toxicology, troponin, beta HCG, EKG) Maintenance studies: BCP, magnesium, phosphorus q3-4 hours Potassium Management: K < 3.3 Meq/l correct BEFORE starting insulin infusion (rule out anuria) Anticipate total body depletion (unless advanced CKD, ARF, ESRD) DKA Fluid management: Start IVF 0.9% saline 10-20 ml/kg in 1st hour, then per MD orders Adjust IVF for shock, ESLD, ESRD, ARF, CHF DKA insulin management: Start insulin 0.1 u/kg IV bolus, 0.1 u/kg/hour IV infusion (See titration tablets over) Once glucose < 250mg/dl: Change to D5 0.45% NS suggested rate 125-200 cc/hour Consider no insulin bolus with HHS Oral intake: May eat if alert and no aspiration risk. Provide SQ rapid acting insulin: Rapid acting SQ 0.3 u/kg divided ⅓ with meals or default insulin: carbohydrate ratio 1:15 male, 1:10 males DKA resolution: Anion gap <=12, Bicarbonate > 18 Meq/l, pH > 7.3, BHB=0 HHS: IVF: Start with 0.9% NaCl 1-1.5L, switch to 0.45% if osmolarity not falling on 0.9% 1-2 L/hour 0.9% NaCl for shock otherwise 500 ml/hour x 4 hours, then 250 ml/hour Insulin: start 0.1 u/kg/hour once osmolarity stops falling with IVF, double if not falling 50-70 mg/dl/hour, decrease 0.02-0.05 u/hour glucose <250-300 mg/dl OR per order sets Water deficit: current TBW x (serum Na/140-1). TBW 50% range lean body weight Corrected sodium: Serum Na Meq/L + glucose (mg/dl)/18 Lower sOsm 3 Mosm/kg/hour. Glucose 50-90 mg/dl/hour maximum Chronic hypernatremia (no hyperglycemia): goal lower by 10Meq/L in 24 hours Transition from IV to SQ insulin post DKA): DKA resolution, stable infusion for at least 4 hours preferable (ideally < 2 units per hour, glucose values between 140-180 mg/dl) and stable IV insulin infusion dose for at least 4-6 hours) Predictors of unsafe transition: wide fluctuations in IV infusion rate High infusion rates (> 2 u/hour) (unless known insulin resistance present) Avoid rebound DKA by giving basal insulin SQ and waiting at least 2 hours (can bridge with SQ rapid acting insulin with 10% of basal dose, if needed) Basal: Check home dose and weight based dose and compare with 50% of 24 hour stable infusion rate (minimum 4 hours) OR consider default of 0.3 u/kg/day glargine, stop IV 2 hours after SQ basal. Total daily dose 0.2-0.8+ u/kg (usually 50% basal and 50% divided between meals). (Alternative: Stop IV infusion after basal PLUS 10% of basal dose as rapid acting SQ) Meal insulin: =basal dose ⅓ with each meal OR insulin: carbohydrate ratio (Default 1:10 males 1:15 females) Some protocols have used 80% of infusion rate to predict insulin needs (be careful to distinguish between basal insulin dose and total daily dose (includes meal insulin). Transition from IV to SQ insulin in critical illness: As above for DKA In some instances best to use steady state insulin infusion rate as predictor of total daily dose (NOT just basal) (may then be divided between basal (usually 50% of total daily dose) and meal insulin. If in doubt, generally default to lower of dose predicted by stable infusion rate OR weight based prediction to minimize the risk of hypoglycemia ALWAYS factor in clinical status: known diabetes, steroid dose changes, fluxes in renal function, degree of stress, glucose control prior to admission (high A1c supports preceding poor glucose control and glucose toxicity), tube feeds, TPN, NPO etc. Consider use of software guided dosing (Endotool implementation in progress) Johns Hopkins Extreme Hyperglycemia Protocol to consider adapting Correction: 1:41-45, 1:31 1:18, 1:12
|
|
LINKED FILES
https://drive.google.com/drive/folders/1S6uX8uoLbc1MsA2GRj8y_0adELiRI_fC?usp=sharing
Protocol: SGL2i use in high risk CV/CHF type 2 diabetes patients
Rationale: Empaglflozin (Empa-Reg) trial showed addition of Jardiance to type 2 patients with CV disease and standard of care, lowers risk of CHF admissions, progression of renal disease and lowers risk of cardiovascular death (FDA indication for this purpose). The Canvas trial with canaglflozin (Invokana) also had CV, CHF and renal benefits and now has an FDA indication for a composite end point of non-fatal stroke, MI and CV death.
Patient selection: Type 2 diabetes + CVD/CHF + eGFR > 45 (studied to 30 in CV outcome trials) (+ adherent to follow up + access to medication)
Contraindication: allergy or eGFR < 45 (consider <30)
Alternatives: Consider GLP1 analog as alternative OR in addition. LEADER, SUSTAIN and REWIND trials show positive CV effects, weight loss (See GLP1 analog cardiometabolic protocol). Consider pioglitazone (Proactive trial, IRIS trial) in select patients.
Precautions: Frequent or severe UTI risk, urinary incontinence/severe polyuria/nocturia/symptomatic BPH, DKA risk: history of DKA, LADA diabetes (Anti-GAD antibody positive, DM1), A1c > 11.5%, marked hyperglycemia symptoms (consider insulin titration first), ? active bladder cancer (questionable signal with dapagliflozin, lower extremity amputation risk (severe PVD, prior amputation, active foot infection (safety signal with canagliflozin and ertugliflozin)).
Volume depletion prevention:
Hold for dehydration (prior to procedures, gastroenteritis, hot environment). Encourage adequate fluid intake.
Inpatient initiation and transition of care:
Jardiance on formulary at LFH, restricted to Endocrinology currently
Agreement to start therapy needed from Cardiology and Endocrinology; primary care and nephrology as needed
Default will be Jardiance (currently best balance or risk/benefit), Invokana is reasonable evidence based alternative
Boehringer Ingelheim offers a transition of care program that includes 30 days free
Transition of care follow up of volume, BP, renal function/electrolytes, diuretic and BP active medication adjustments per Cardiology, glucose monitoring and adjustment of diabetes medications per endocrinology (or primary care).
Link to Google Drive Files drive.google.com/open?id=1tjbH2OEJfKlIs02Mr_-syi4jdCTv49RV
